A.B.C. of Acid Base Disorders
deopujari.com for details
Blood gas abnormalities form an integral part of assessment of critically ill patients and deserve an important place in their management. Fear of proper analysis of blood gases is universal and this is an attempt to simplify the approach to blood gas analysis and especially the underlying mathematics.
Acid : Is a substance, which can donate H+ ion. H+ ion, is also known as a proton. Hydrogen atom is made of a proton and an electron revolving around it. Loss of electron from this atom leaves a proton (H+).
Base: Is a substance that can accept a proton e.g. OH- ions combines with H+ ions to form water, thus OH- ions are a base.
The concept of pH.
Concentration of H+ ions in a solution can be conveniently considered in two forms, in the form of nanomoles / lit or in the form of pH (pH is negative log of H+ ion concentration)
As is obvious from the above equation, if the concentration of H+ ion increases the pH will decrease. Normal H+ ion concentration is 40 nanomoles / liter. This corresponds to pH of 7.40 (Mnemonic 7.40 and 40 nanomoles /lit.)
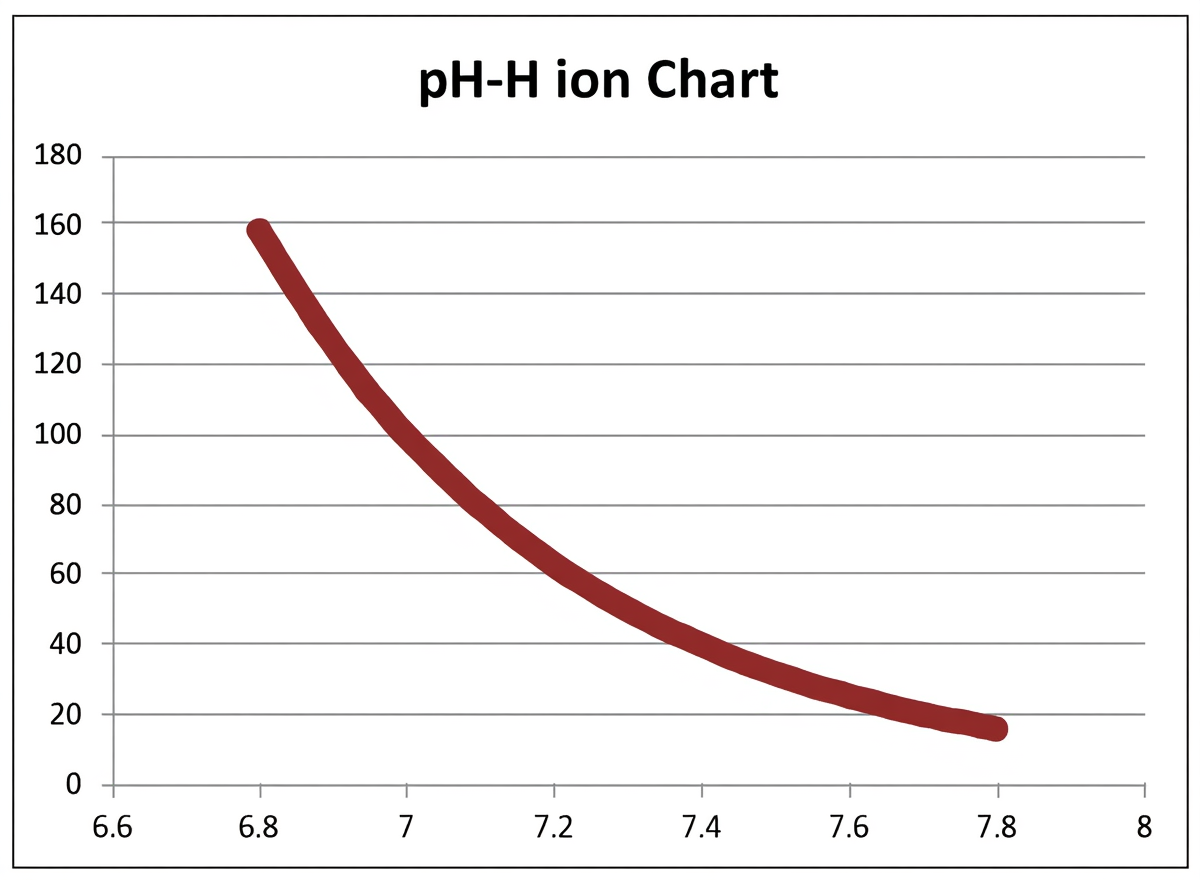
Fig. 1: pH and H+. Change in pH with change in H+ ion concentration. Change is inversely proportional.
pH as a ratio:
The essence of understanding acid base disorders lies in realization of the fact that pH is a ratio between acid and base. Normal pH means normal ratio between acid and base in the body. Bicarbonate buffer system in the body will explain the above statement. The ratio between bicarbonate and carbonic acid is 20:1, and at this ratio the pH is normal. Addition or deletion of acid or alkali will alter the ratio and thus the pH, body tries to normalize the ratio and in turn the pH (Compensation).
The Metabolic and Respiratory components
Any change in pH that occurs because of bicarbonate is called as metabolic change, the change occurring because of PaCO2 is called as respiratory change. Thus we have respiratory and metabolic acidosis and alkalosis. One must remember that bicarbonate changes pH in the same direction (increase in bicarbonate will increase pH and decrease in bicarbonate will decrease pH) and PaCO2 changes pH in opposite direction.
↓ PaCO2 → ↑ pH
↑ HCO3- → ↑ pH
Fig. 2: Co-relation between pH and HCO3- and pH and PaCO2
Lungs primarily control respiratory component in body and metabolic component is controlled by kidneys. Thus pH is a ratio between renal and pulmonary functions. Carbon dioxide in the body behaves like an acid and thus when accumulates we call it as respiratory acidosis and when PaCO2 levels are low as respiratory alkalosis.
Compensation:
With primary alteration in respiratory system (hypo or hyperventilation) body compensates by altering the metabolic component (Renal). With primary alteration in metabolic system (Bicarbonate) body compensates by altering the respiratory component (PaCO2). Renal compensation takes several days, respiratory compensation occurs in hours.
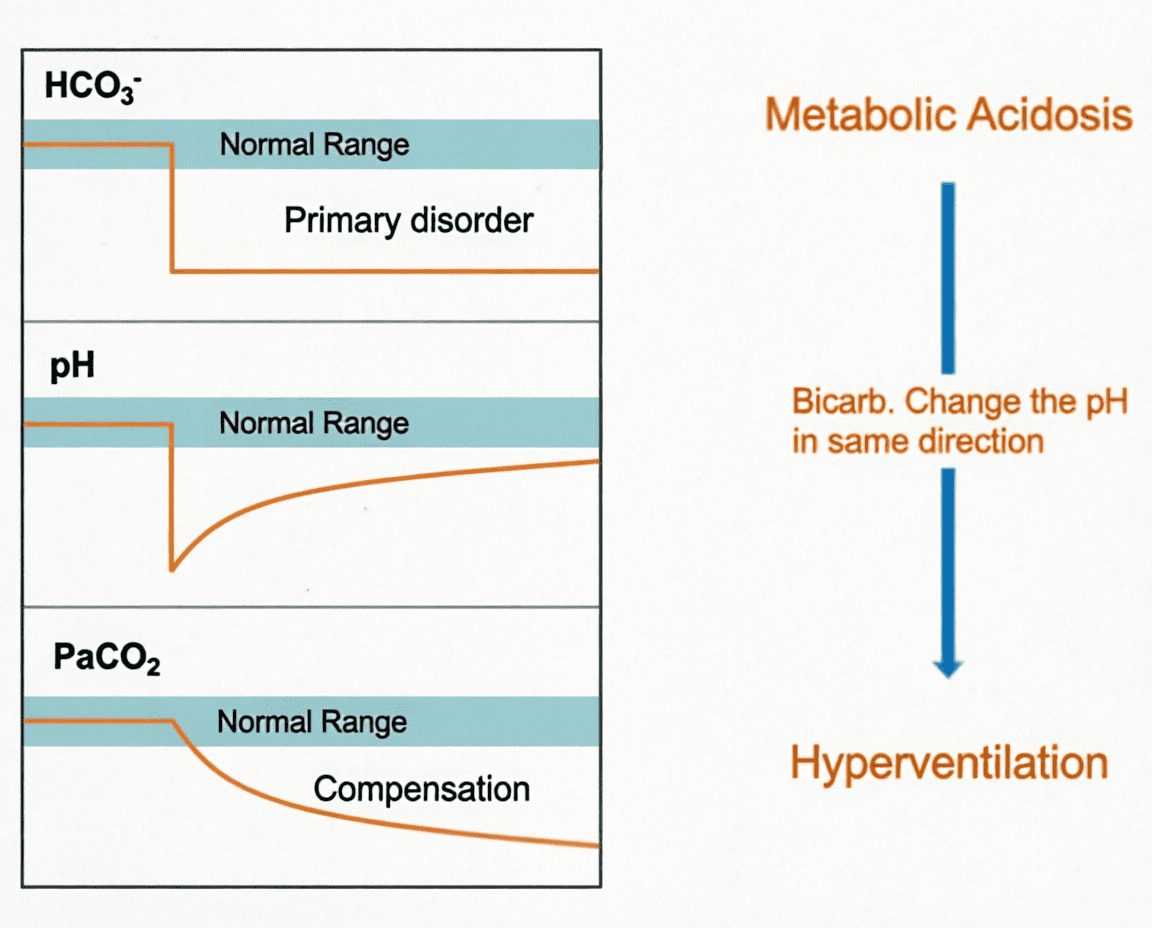
Fig. 3 : Metabolic acidosis.
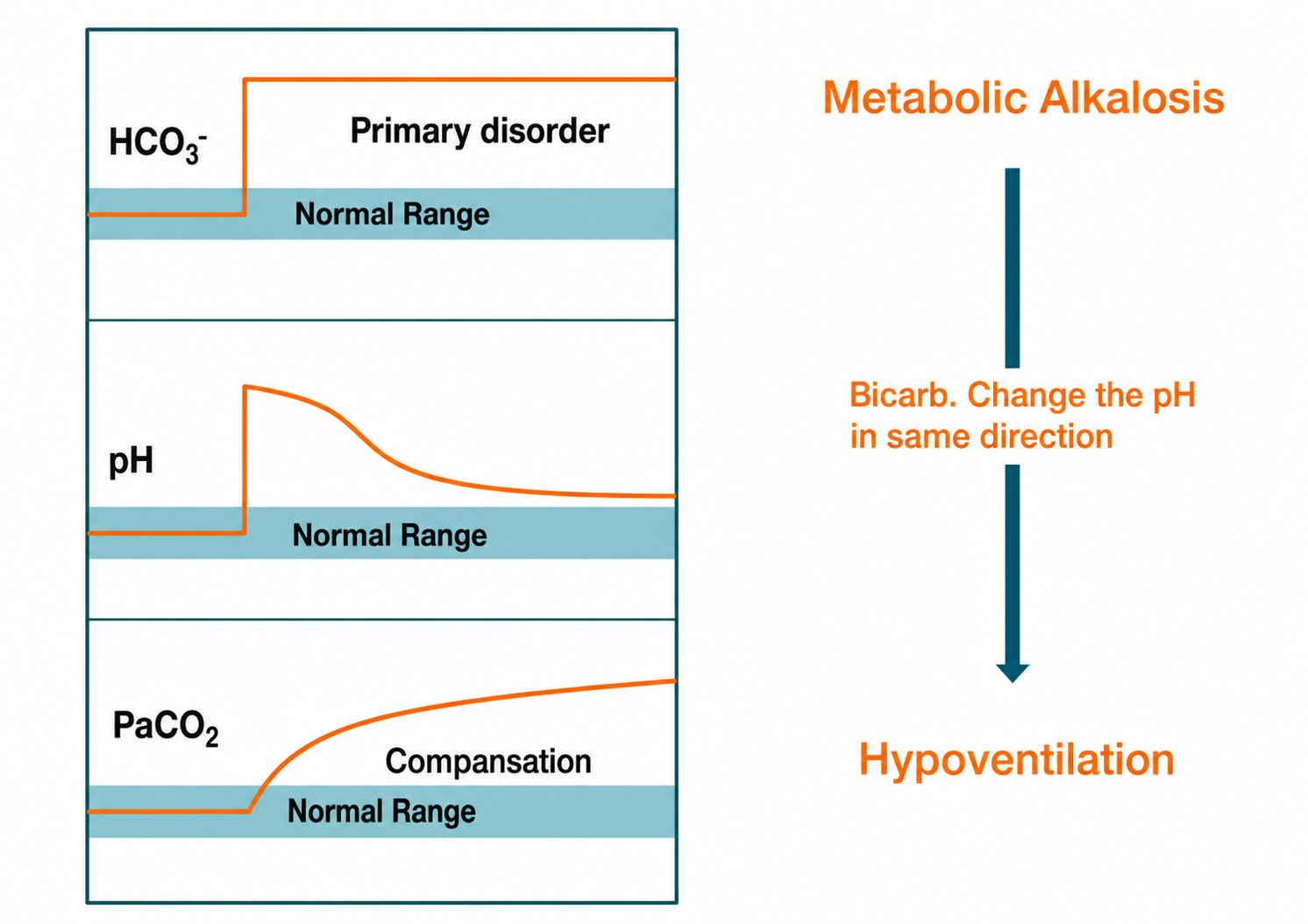
Fig. 4: Metabolic alkalosis.
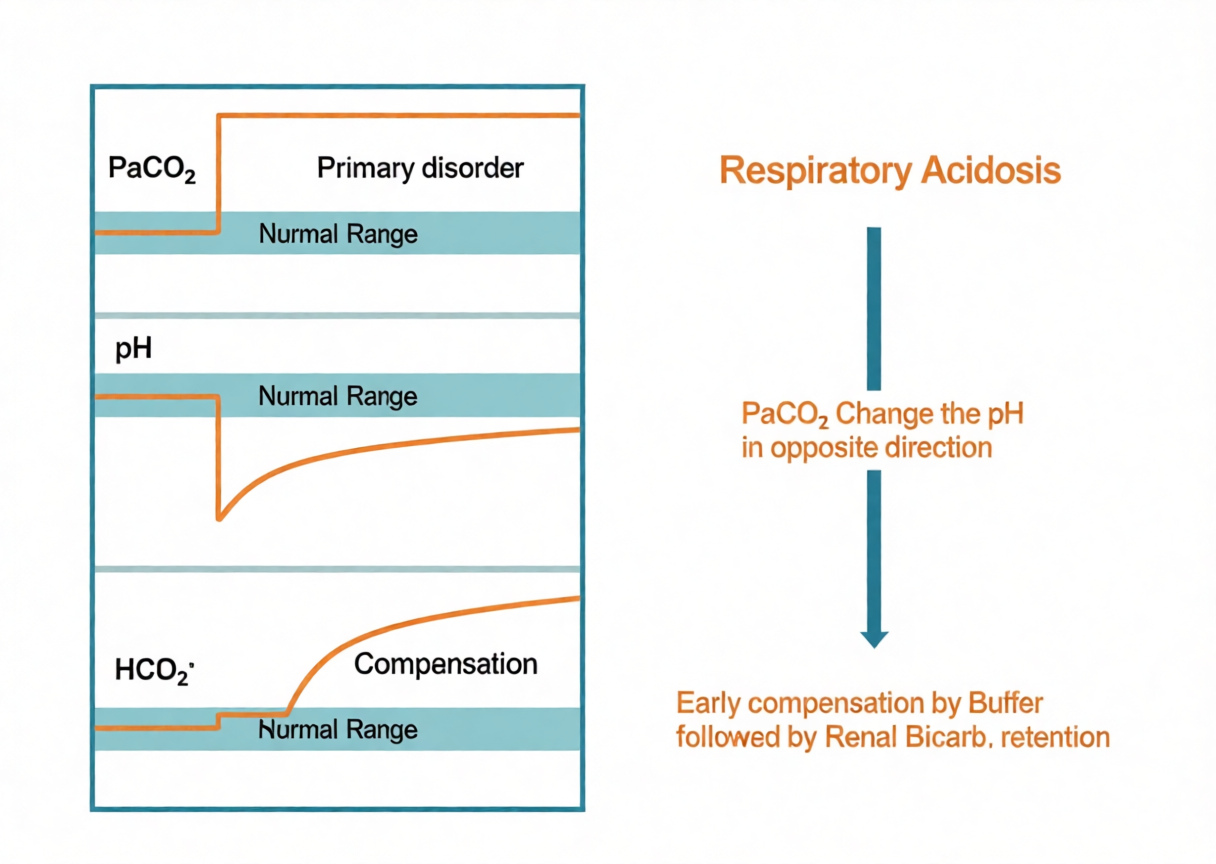
Fig. 5 : Respiratory acidosis.
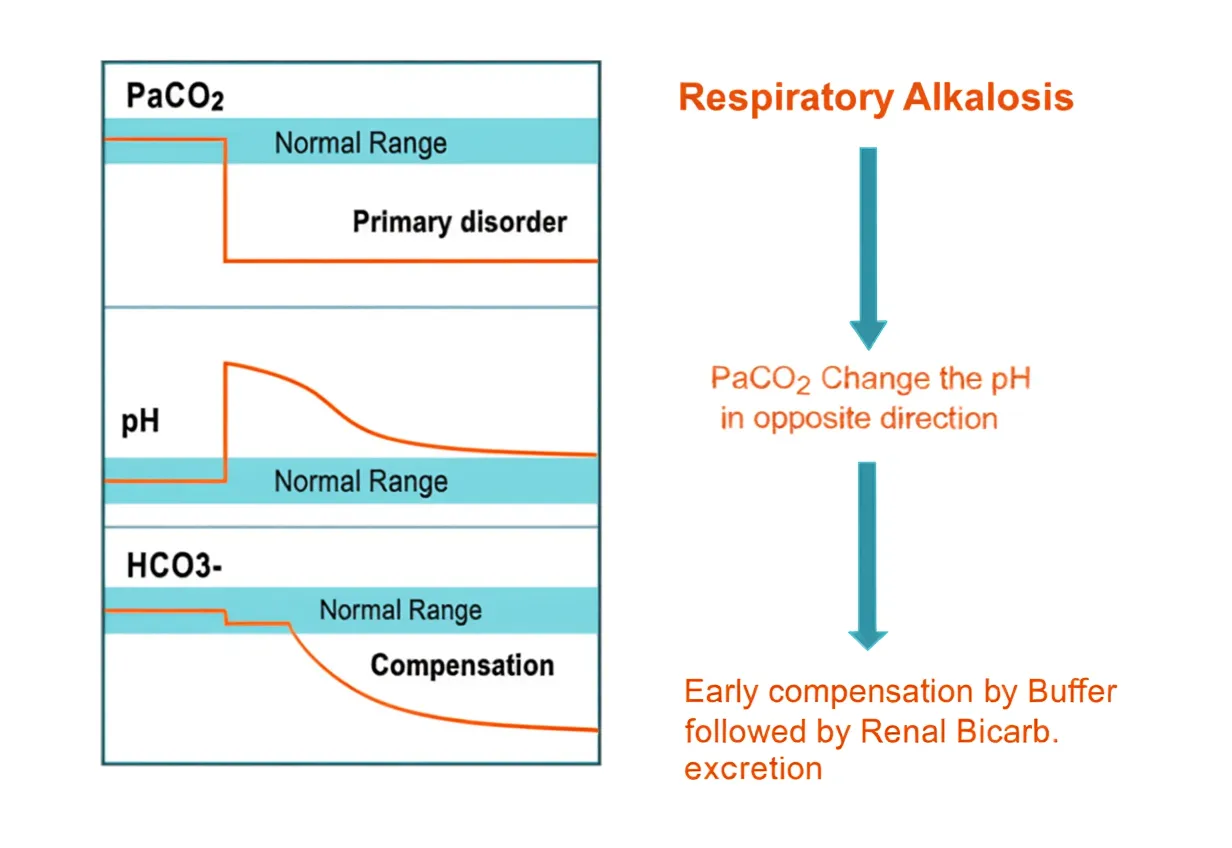
Fig. 6 : Respiratory alkalosis.
Practical approach to ABG report:
Look at the three values for rapid analysis of ABG.
- pH
- PaCO2
- HCO3- (Calculated parameter)
HCO3- is calculated on the basis of values of pH and PaCO2, using simplified form of Henderson-Hasselbalch (HH) equation.
Steps for interpretation of ABG:
Step 1...
Look at the pH : Is the value abnormal ?
Normal 7.35 to 7.45
Below 7.35 is Acidemia
Above 7.45 is Alkalemia
Normal pH does not rule out an ABG abnormality.
Step 2....
What is responsible for the change in pH ?
Look for Bicarbonate : Is the value abnormal ?
IF BICARBONATE IS PRIMARILY RESPONSIBLE for the change in pH, then the pH will change in the direction of the change in bicarbonate. (Low bicarbonate should lower pH and high bicarbonate will increase pH)
Look for PaCO2 value : Is the value abnormal ?
IF CARBON DIOXIDE IS PRIMARILY RESPONSIBLE for the change in pH, then the pH will change in opposite direction of the change in PaCO2.
At the end of this step, primary ABG abnormality is diagnosed.
e.g. :
pH low (Acidemia) with
Low bicarbonate + Metabolic acidosis
OR
High PaCO2 + Respiratory acidosis.
pH high (Alkalemia) with
High bicarbonate + Metabolic alkalosis
OR
Low PaCO2 + Respiratory alkalosis
Figure 7. Conceptual co-relation between pH and PaCO2.
Step 3 ....
Look for compensation
Metabolic acidosis
If actual PaCO2 is more than expected PaCO2
+ Additional Respiratory Acidosis.
If actual PaCO2 equals expected PaCO2
+ Compensated Metabolic Acidosis
If actual PaCO2 less than expected PaCO2
+ Additional Respiratory Alkalosis.
Metabolic alkalosis
If actual PaCO2 more than expected PaCO2
+ Additional Respiratory Acidosis.
If actual PaCO2 equals expected PaCO2
+ Compensated Metabolic Acidosis
If actual PaCO2 less than expected PaCO2
+ Additional Respiratory Alkalosis.
Respiratory acidosis
Compensation in respiratory abnormality can be judged by correlating change in HCO3- with change in PaCO2.
With every 10mm Hg increase in PaCO2 above 40, increase in HCO3-
| By less than 1 | + Additional metabolic acidosis |
| By 1 | + Acute respiratory acidosis |
| By >1 to <4 | + Partially compensated respiratory acidosis. |
| By 4 to 5 | + Chronic respiratory acidosis |
| By more than 5 | + Additional metabolic alkalosis |
Respiratory alkalosis
With every 10 mm Hg decrease in PaCO2 below 40, decrease in HCO3-
| By less than 2 | + Additional metabolic alkalosis |
| By 2 | + Acute respiratory alkalosis |
| By >2 to <4 | + Partially compensated respiratory alkalosis |
| By 4 to 5 | + Chronic respiratory alkalosis |
| By more than 5 | + Additional metabolic acidosis |
Limits of Compensation
For any acid-base abnormality compensation is an expected reaction but there is a limit to which compensation can extend. Compensation beyond the expected limits suggest an additional acid base abnormality.
Limits of compensation...
| Metabolic acidosis | Lowest expected PaCO2 = 10 |
| Metabolic alkalosis | Highest expected PaCO2 = 60 |
| Respiratory acidosis | Highest expected HCO3- = 35 |
| Respiratory alkalosis | Lowest expected HCO3- = 13 |
(Limits of compensation may vary ±2)
Step 4....
Clinical correlation
No arterial blood gas assessment is complete without clinical correlation.
Step 5....
Further evaluation
Metabolic acidosis:
ANION GAP (Normal is 8 to 12) Anion gap = Na – (Cl + HCO3-)
Low anion gap (less than 8)
Laboratory error, Lithium, Bromide or Iodide intoxication, Polyclonal gammopathy, Hypercalcemia, Hypermagnesemia, Polymyxin B (as a chloride than sulfate).
Normal anion gap
Look for urinary anion gap
Urinary Anion Gap = Urinary Na + Urinary K – Urinary Cl
a. Urinary anion gap : Negative
Diarrhea, Evaluate for Proximal RTA
b. Urinary anion gap : Positive
Evaluate for RTA type I or type IV
High anion gap
Measure Delta-Delta and Osmolar gap
Delta-delta is
+ − 5 to 5 High anion gap acidosis,
+ more than 5 High anion gap acidosis with metabolic alkalosis
+ less than −5 High anion gap acidosis with normal anion gap acidosis
OSMOLAR GAP
Osmolar gap = Measured Osmolarity - Calculated Osmolarity
Osmolar gap more than 10 (more than 20 in elderly) suggests Toxic alcohol ingestion.
Metabolic alkalosis:
Categorize depending on urinary chloride level.
1) Urinary chloride less than 25 mmol /L: Saline responsive
+ Gastrointestinal fluid loss
+ Milk Alkali Syndrome. (Hypercalcemia with Renal Failure)
2) Urinary chloride more than 40 mmol /L: Saline unresponsive
(Rule out Diuretic use or magnesium deficiency)
Measure urinary Potassium
a. Less than 20 mmol /day: laxative abuse
b. More than 30 mmol /day: Measure blood pressure
+ Low or normal BP: Gitelman's Syndrome (Low Urinary Calcium)
OR Bartter's Syndrome (High Urinary Calcium)
+ High Blood pressure: Mineralocorticoid excess (usually with hypokalemia)
Crux of complete ABG analysis:
All the blood gas reports need to be seen in respect with the electrolytes, oxygenation status, clinical condition of the patient and the earlier reports of blood gases. Single report may fail to give the complete clinical picture of the patient and thus needs to be evaluated in holistic view.
From the desk of .....
Dr Lawrence Martin
Calculated bicarbonate reported with the
ABG Vs Measured bicarbonate from a venous blood sample.
Comparison is often made between the calculated bicarbonate reported with the ABG, and the measured bicarbonate from a venous blood sample. These two HCO3- values should be within a few mEq/L of each other but are not identical, for several reasons.
- The ABG bicarbonate is a calculated value from the Henderson-Hasselbalch equation and the measured PaCO2 and pH. Venous HCO3- is a laboratory measurement (part of serum electrolytes), and also includes a contribution from dissolved CO2, which is 1-2 mEq/L. Thus you are comparing a calculation on one part of the circulation with a measurement from another part of the circulation.
- If a tourniquet is used to draw the venous sample, that might affect the HCO3- value.
- An ABG blood sample is tested within minutes of being drawn, but a venous sample may sit around, which could affect the HCO3- measurement.
Continued...
- The two samples - venous and arterial - are often drawn at different times, and under different clinical circumstances, especially for acutely ill patients. Acute changes in blood gases and electrolytes could account for a discrepancy.
In summary, expect a difference between the calculated HCO3- from the ABG and the measured HCO3- from venous blood. In a stable clinical situation, the difference is typically 1- 4 mEq/L, but can be up to 6 mEq/L. If the difference is larger, and/or you have a reason to question the results, then consider repeating one or both the tests (ABG and/or venous electrolytes).